![[advertisement] concertmedical](../files/bk-nysora-ad.jpg)
Ultrasound-Guided Fascia Iliaca Block
Figure 1: Needle insertion for the fascia iliaca block. The black dot indicates the position of the femoral artery. Essentials
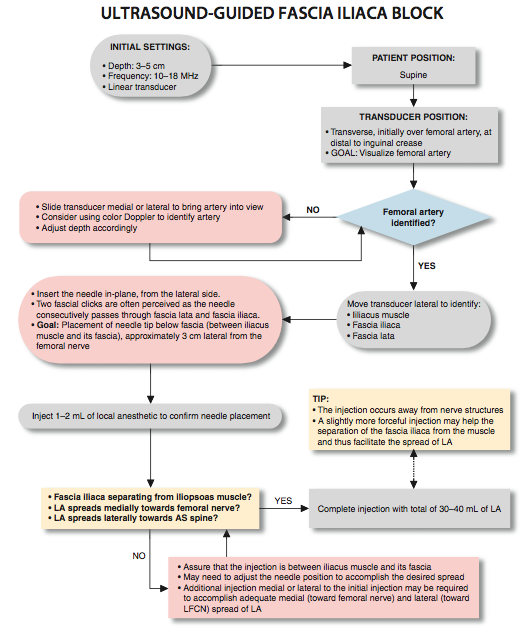
General Considerations Fascia iliaca block is a low-tech alternative to a femoral nerve or a lumbar plexus block. The mechanism behind this block is that the femoral and lateral femoral cutaneous nerves lie under the iliacus fascia. Therefore, a sufficient volume of local anesthetic deposited beneath the fascia iliaca, even if placed some distance from the nerves, has the potential to spread underneath the fascia and reach these nerves. Traditionally, it was believed that the local anesthetic could also spread underneath fascia iliaca proximally toward the lumbosacral plexus; however, this has not been demonstrated consistently. The non-ultrasound technique involved placement of the needle at the lateral third of the distance from the anterior superior iliac spine and the pubic tubercle, using a "double-pop" technique as the needle passes through fascia lata and fascia iliaca. However, block success with this "feel" technique is sporadic because false "pops" can occur. The ultrasound-guided technique is essentially the same; however, monitoring of the needle placement and local anesthetic delivery assures deposition of the local anesthetic into the correct plane. Ultrasound Anatomy The fascia iliaca is located anterior to the iliacus muscle (on its surface) within the pelvis. It is bound superolaterally by the iliac crest and medially merges with the fascia overlying the psoas muscle. Both the femoral nerve and the lateral cutaneous nerve of the thigh lie under the iliacus fascia in their intrapelvic course. Anatomic orientation begins in the same manner as with the femoral block: with identification of the femoral artery at the level of the inguinal crease. If it is not immediately visible, sliding the transducer medially and laterally will eventually bring the vessel into view. Immediately lateral and deep to the femoral artery and vein is a large hypoechoic structure, the iliopsoas muscle (Figure 2). It is covered by a thin layer of connective tissue fascia, which can be seen separating the muscle from the subcutaneous tissue superficial to it. The hyperechoic femoral nerve should be seen wedged between the iliopsoas muscle and the fascia iliaca, lateral to the femoral artery. The fascia lata (superficial in the subcutaneous layer) is more superficial and may have more then one layer. Moving the transducer laterally several centimeters brings into view the sartorius muscle covered by its own fascia as well as the fascia iliaca. Further lateral movement of the transducer reveals the anterior superior iliac spine (Figure 2). Distribution of Blockade The distribution of anesthesia and analgesia that is accomplished with the fascia iliaca block depends on the extent of the local anesthetic spread and the nerves blocked. Blockade of the femoral nerve results in anesthesia of the anterior and medial thigh (down to and including the knee) and anesthesia of a variable strip of skin on the medial leg and foot. The femoral nerve also contributes to articular fibers to both the hip and knee. The lateral femoral cutaneous nerve confers cutaneous innervation to the anterolateral thigh. 
Figure 2: A panoramic view of ultrasound anatomy of the femoral (inguinal) crease area. From lateral to medial shown are tensor fascia lata muscle (TFLM), sartorius muscle (SaM), Iliac muscle, fascia iliaca, femoral nerve (FN), and femoral artery (FA). The lateral, middle and medial 1/3s are derived by dividing the line between the FA and anterior-superior iliac spine in three equal 1/3 sections.
Equipment Equipment needed includes the following:
Landmarks and Patient Positioning This block is typically performed with the patient in the supine position, with the bed or table flattened to maximize access to the inguinal area (Figure 3). Although palpation of a femoral pulse is a useful landmark, it is not required because the artery is quickly visualized by placement of the transducer transversely on the inguinal crease, followed by slow movement laterally or medially.
Technique With the patient in the proper position, the skin is disinfected and the transducer positioned to identify the femoral artery and the iliopsoas muscle and fascia iliaca. The transducer is moved laterally until the sartorius muscle is identified. After a skin wheal is made, the needle is inserted in-plane (Figure 1). As the needle passes through fascia iliaca the fascia is first seen indented by the needle. As the needle eventually pierces through the fascia, pop may be felt and the fascia may be seen to "snap" back on the ultrasound image. After negative aspiration, 1 to 2 mL of local anesthetic is injected to confirm the proper injection plane between the fascia (Figure 4) and the iliopsoas muscle (Figure 5A, B, and C). If local anesthetic spread occurs above the fascia or within the substance of the muscle itself, additional needle repositions and injections may be necessary. A proper injection will result in the separation of the fascia iliaca by the local anesthetic in the medial-lateral direction from the point of injection as described. If the spread is deemed inadequate, additional injections laterally or medially to the original needle insertion or injection can be made to facilitate the medial-lateral spread. In an adult patient, between 30 and 40 mL of local anesthetic is usually required for successful blockade. The success of the block is best predicted by documenting the spread of the local anesthetic toward the femoral nerve medially and underneath the sartorius muscle laterally. In obese patients, an out of plane technique may be favored. The block should result in blockade of the femoral in all instances (100%) and lateral femoral nerve (80%-100%). Block of anterior branch of the obturator nerve is unreliable with fascia iliaca block.
Figure 5: (A) Path of the needle for the fascia iliaca block. The needle (1) is shown underneath the fascia iliaca lateral to the femoral artery (not seen) but not too deep to be lodged into the iliac muscle. (B) A simulated spread (area shaded in blue) of the local anesthetic to accomplish a fascia iliaca block. (C) Spread of the local anesthetic (LA) under the fascia iliaca. Some local anesthetic is also seen deep within the iliacus muscle (yellow arrows). When this occurs, the needle should be pulled back more superficially. (D) Extension of the LA laterally underneath the sartorius muscle. Some LA fills the adipose tissue between fascia iliaca and iliacus muscle (yellow arrows).
  |
More from Updates


Neurologic Complications of Peripheral Nerve Blocks
Author: Jeff Gadsden Nerve injury following peripheral nerve blockade (PNB) is a potentially devastating complication that ...





| 02/20/2016(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/23/2016 | |
| 10/01/2024 |
admin
- Anatomy of Nerve Blockade
- Ultrasound-Guided Interscalene Brachial Plexus Block
- Ultrasound-Guided Popliteal Block
- Ultrasound-Guided Supraclavicular Brachial Plexus Block
- Ultrasound-Guided Fascia Iliaca Block
- Ultrasound-Guided Femoral Nerve Block
- Neurologic Complications of Peripheral Nerve Blocks
- Ultrasound-Guided Interscalene Brachial Plexus Block
- Ultrasound-Guided Axillary Brachial Plexus Block
![[advertisement] gehealthcare](../files/banners/banner1_250x600/GEtouch(250X600).gif)
Post your comment