![[advertisement] concertmedical](../../../files/bk-nysora-ad.jpg)
Obturator Nerve Block
Obturator nerve block is used to treat hip joint pain and in the relief of adductor muscle spasm associated with hemi-or paraplegia. Muscle spasticity is relatively common problem among patients suffering from central neurological problems such as cerebrovascular pathology, medullar injuries, multiple sclerosis, infantile cerebral palsy, etc.
|
Introduction Selective obturator nerve block was first described by Labat in 1922.[1] More interest in obturator nerve block emerged a few years later when Pauchet, Sourdat and Labat stated that "obturator nerve block combined with blocks of the sciatic, femoro-cutaneous nerves, anesthetized the entire lower limb". However, a lack of clear anatomical landmarks, the block complexity and inconsistent results were the reasons why this block had been used infrequently. Historically, Labat's classical technique remained forgotten until 1967 when it was modified by Parks.[2] In 1993 the inter-adductor approach was described by Wassef,[3] which was further modified by Pinnock in 1996.[4] In 1973, Winnie introduced the concept of the "3-in-1 block", an anterior approach to the lumbar plexus using a simple paravascular inguinal injection to anesthetize the femoral, lateral cutaneous nerve of the thigh (LCN) and obturator nerves.[5] Since its description however, multiple studies refuted the ability of the "3-in-1 block" to reliably block the obturator nerve with this technique. However, with the introduction of modern nerve stimulators, selective blockade of the obturator nerve has become more reliable and has seen a resurgence of interest in recent times. Indications Obturator nerve block is used to treat hip joint pain and in the relief of adductor muscle spasm associated with hemi-or paraplegia. Muscle spasticity is relatively common problem among patients suffering from central neurological problems such as cerebrovascular pathology, medullar injuries, multiple sclerosis, infantile cerebral palsy, etc. Spasticity of the adductor muscle induced via the obturator nerve, plays a major role in associated pain problems and makes patient grooming and mobilization very difficult. Tenotomies, cryotherapy, botulin toxin infiltration, surgical neurolysis and muscle interpositions have been suggested to remedy this problem.[6,7,8,9] A number of diagnostic or therapeutic procedure on the knee and thigh can be performed by combining obturator nerve block with block of the sciatic, LCN and femoral nerves. Common clinical practice is to combine a sciatic nerve with the femoral nerve block for surgical procedures distal to the proximal one third of the thigh. When deemed necessary, addition of a selective obturator nerve block may reduce intraoperative discomfort, improve tourniquet tolerance and improve the quality of postoperative analgesia in these cases. Obturator nerve block is also occasionally used in urological surgery to suppress the obturator reflex during transurethral resection of the lateral bladder wall. Direct stimulation of the obturator nerve by the resector as it passes in close proximity to the bladder wall results in a sudden, violent adductor muscle spasm. This is not only distracting to the surgeon, but also potentially dangerous, increasing the risk of serious complications such as bladder wall perforation, vessel laceration, incomplete tumor resection and obturator hematomas etc.[10,11] Prevention strategies include muscle relaxation, reduction in the intensity of the resector, the use of laser resectors, shifting to saline irrigation, peri-prostate infiltrations and/or endoscopic transparietal blocks[13-16] However, a selective obturator nerve block still remains the safest and most effective alternative to this problem.[17-22]
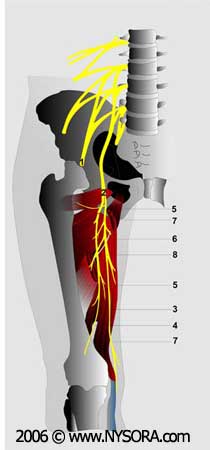
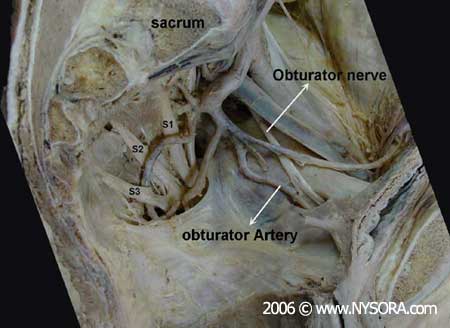
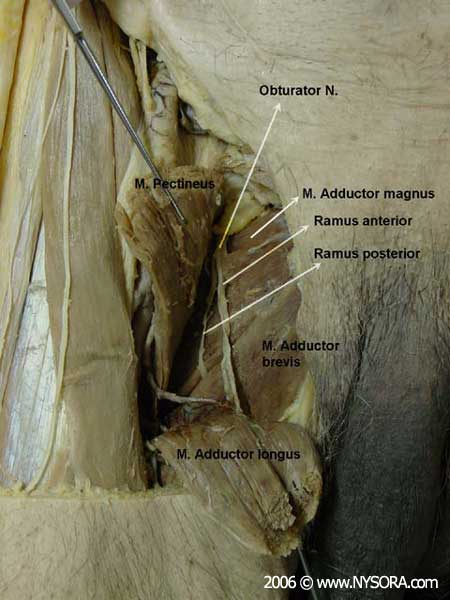
Neurolytic blockades with alcohol or phenol, performed with the help of a nerve stimulator and/or radioscopy, result in a cost-effective and effective reduction of muscle spasms.[23-28] The main drawback is its temporal duration and the need to repeat the blockade when the previous block wears off. Selective obturator nerve block has also been used in the diagnosis and treatment of chronic pain states secondary to knee arthrosis or pelvic tumors resistant to conventional analgesic approaches.[29-33] Contraindications Patient refusal, presence of inguinal lymphadenopathy, perineal infection or haematoma at the needle insertion site are all contraindications to obturator nerve blockade. The presence of a pre-existing obturator neuropathy, clinically manifested by groin pain, pain of the posteromedial aspect of the thigh and occasionally, paresis of the adductor group of muscles, are relative contraindications to this block. Obturator nerve blocks should be avoided in the presence of a coagulopathy. Anatomy The obturator nerve is a mixed nerve which in most cases, provides motor function to the adductor muscles and cutaneous sensation to a small area behind the knee. It is derived from the anterior primary rami of L2, L3 and L4, Figure 1. On its initial course, it runs within the psoas major muscle. Taking a vertical course, it emerges from the inner border of the psoas, staying medial and posterior at the pelvis until it crosses at the level of the sacroiliac joint (L5), under the common iliac artery and vein and runs anterior/lateral to the ureter, Figure 2. At this level, it courses close to the wall of the bladder on its inferior/lateral portion and then it takes place anterior to the obturator vessels within the superior part of the obturator foramen, exiting the pelvis below the pubic superior branch. In its intrapelvic course, the obturator nerve is separated from the femoral nerve by the iliopsoas muscle and iliac fascia. It innervates the parietal peritoneum on the lateral pelvic wall and contributes collateral branches to the obturator externus muscle and the hip joint. It leaves the pelvis by passing through the obturator canal before entering the adductor region of the thigh, Figure 3. Here, 2.5 - 3.5 cm after leaving the obturator foramen, the obturator nerve devides into its two terminal branches, anterior and posterior, providing innervation to the hip adductor compartment, (Figure 3).[34]
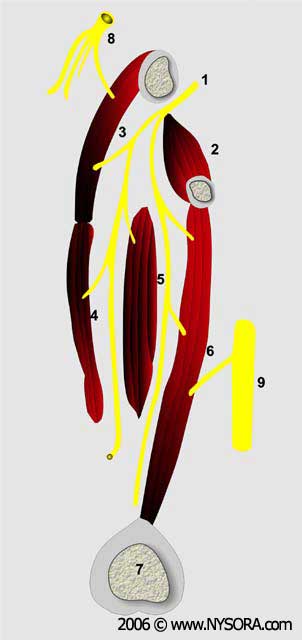
The anterior branch descends behind the pectineus and adductor longus, and in front of the obturator externus and adductor brevis. It gives muscular branches to the adductor longus, adductor brevis, gracilis and occasionally the pectineus, and terminates as a small nerve that innervates the femoral artery, Figure 4. In 20% of subjects, it contributes a branch which anastamoses with branches of the femoral nerve, forming the subsartorial plexus, from which sensory branches emerge to supply sensation to posteromedial aspect of the inferior third of the thigh. The anterior branch contributes articular branches to anteromedial aspect of the hip joint capsule (Figure 5) but does not innervate the knee joint. The posterior branch descends between the adductor brevis in front, and the adductor magnus behind. It terminates by passing through the adductor hiatus to enter the popliteal fossa supplying the posterior aspect of the knee joint and the popliteal artery. During its course, the posterior branch sends muscular branches to the obturator externus, the adductor magnus and occasionally the adductor brevis muscles (Figure 4).
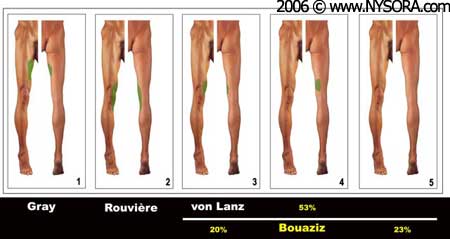
Cutaneous innervation by the obturator nerve varies according to the authors and is illustrated in Figure 6.
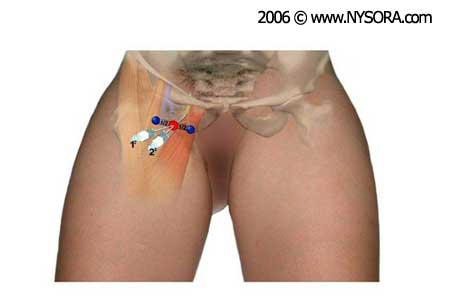
Anatomical variants There are numerous variations to the formation, course and distribution of the obturator nerve which can have clinical implications. For instance, in 75% of cases, the obturator nerve divides into its two terminal branches as it passes through the obturator canal. In 10% of cases this division occurs before the nerve reaches the obturator canal, and in the remaining 15% of cases, after entering the thigh. Occasionally, the anterior and posterior branches descend through the thigh behind the adductor brevis. Importantly, the sensory cutaneous branch of the obturator nerve is often absent. Up to 20% of subjects possess an accessory obturator nerve which can be formed from variable combinations of the anterior rami L2-L4 or emanate directly from the trunk of the obturator nerve.[35] It accompanies the obturator nerve as it emerges from the medial border of the psoas but unlike the obturator, passes in front of the superior pubic ramus to supply a muscular branch the pectineus. It contributes articular branches to the hip joint and terminates by anastomosing with the obturator nerve itself. Equipment To perform a block, the following equipment is required: Landmarks 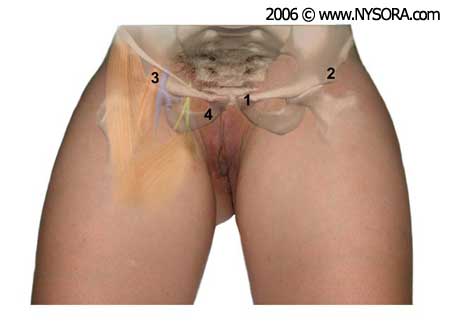 Figure 7. Anatomical landmarks for the blockade of the obturator nerve. 1. pubic tubercle; 2. Anterio-superior iliac spine; 3. femoral artery; 4. tendon of the long adductor muscle. Anatomical landmarks vary depending on the chosen approach. However, it is useful to identify and outline the following landmarks regardless of the approach chosen, (Figure 7): Bony landmarks: Anterior and superior iliac spine and pubic tubercle, inguinal ligament. Vascular landmarks femoral artery, femoral crease Muscular landmarks: tendon of the long abductor muscle Technique There are several methods to accomplish block of the obturator nerve. These approaches can be grouped into plexus block techniques where the obturator nerve is blocked along with other components of the lumbo-sacral plexus and specific single-nerve block techniques for the obturator nerve. Plexus Block Techniques Several different approaches have been described, however, the lumbar plexus block via the posterior approach (in the psoas compartment) is the only technique that ensures an acceptable success rate of obturator nerve blockade. "3 in 1" block technique Based upon the theoretical existence of a suprainguinal compartment, in 1973 Winnie described the lumbar plexus block by an anterior approach or the "3 in 1".[36] According to the "3 in 1" concept, large volume of local anesthetics is injected over the femoral nerve to spread underneath the fascia iliaca. When combined with distal compression, the local anesthetic spreads proximally reaching the lumbar plexus. Unfortunately, several studies have repeatedly failed to demonstrate the reliability of this technique to obtain block of the lumbar plexus or the obturator nerve.[37-40] In addition, studies in human cadavers have documented the absence of a fluid-conducting compartment that would allow such an extensive proximal spread of the local anesthetic.[41] Instead, in cases anesthesia of the cutaneous branches of the obturator with the "3 in 1" technique is a result of a lateral or distal spread, rather than proximal, as initially thought. Of note, increasing the volume of injectate does not increase the spread toward the lumbar plexus; no differences were found when local anesthetic injection volumes of 20 or 40 ml were compared.[42] Theoretically, catheters inserted by an inguinal approach can ascend toward the psoas compartment, however, only a minor percentage (23%) of catheters can be reliably positioned.[43-45] Iliofascial block technique Dalens first described this approach in 1989 for use in pediatric patients.[46] Following Winnie's reasoning for the "3 in 1" block, he took a more lateral approach and reported a 100% success rate for femoral and femorocutaneous nerve blockade and 88% success rate for the obturator nerve. However, follow up studies in adults did not confirm these results.[47,48] In adults, the iliofascial approach allows more successful block of the lateral femorocutaneous nerve when compared to the "3 in 1" technique, however the obturator nerve remains spared.[49,50] Psoas compartment block Since Winnie's description of the posterior approach to the lumbar plexus in 1974 (psoas compartment block), numerous modifications of the technique have been described.[51-55] The obvious advantage of the lumbar plexus is the ability to obtain a complete lumbar plexus block with a single injection. Indeed, the studies have demonstrated femoral nerve block close to 100% plexus block with this technique, whereas femorocutaneous and obturator nerve blocks are anesthetized 88-93% of the time.[56,57] Parasacral sciatic block Mansour initially described this technique in 1993 with the objective of achieving a more complete sciatic nerve block.[58,59] Since this technique is a true plexus block, it provides more consistent anesthesia of all branches of the sciatic nerve. It successfully blocks the posterior cutaneous nerve of the thigh, the gluteal superior and inferior nerves and the pudendal nerve. Additionally, the splacnic nerves, the inferior hypogastric plexus, the proximal portion of sympathetic trunks and the obturator nerve are located close to the point of injection, thus a blockade of all these nervous structures would be theoretically achievable with a single injection. However, recent anatomical and clinical studies suggest that the parietal peritoneum and the pelvic fascia surrounding the sacral plexus is anatomically separated from the obturator nerve that runs along the medial border of the psoas. Consequently, while the parasacral approach to sciatic nerve block should result in a complete block of the sacral plexus, the obturator nerve may be spared.[60] Selective Block Techniques Labat's classical technique
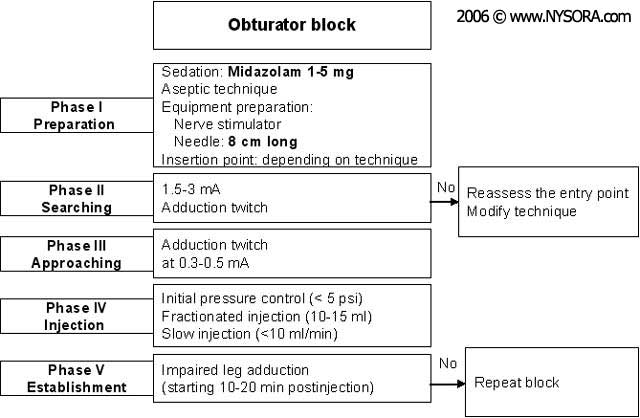
Labat's classical approach was the most popular technique before the development of new approaches - more easily to perform and less uncomfortable to patients. Originally described as a paresthesia method, the advent of nerve stimulation has increased the effectiveness, patient discomfort and reduced complications and number of needle insertions. The procedure sequence consists of five phases, depicted in Figure 8. Nerve stimulation is began using a current of 2-3 mA (2 Hz, 0.1-0.3 msec), and reduced to 0.3-0.5 mA before injection of local anesthetic. The patient lays supine, with the limb to be blocked at 30º abduction. The pubic tubercle is identified by palpation and a 1.5 cm long line is drawn laterally and caudally (the point of injection being at the end of the later). The classical approach consists of carrying out three consecutive movements of the needle until the tip of the needle is placed over the top of the obturator foramen, where the nerve runs before splitting into its two terminal branches. Using a 22G 8 cm long needle, the skin is penetrated perpendicularly and the needle is advanced until it makes contact with the inferior border of the superior pubic branch at a depth of 2-4 cm. During the second phase, the needle is slightly withdrawn and then slipped along the anterior pubic wall (another 2-4 cm); following this it is redirected anterior/posterior. Finally, the needle is withdrawn again and slightly redirected (cephalically and laterally) at an angle of 45º for another 2-3 cm until contractions of the thigh adductor muscles are observed. This technique can be simplified by eliminating the second movement of the needle. Hence, after making contact with the pubic branch, the needle can be redirected 45º laterally to the obturator foramen (Figure 9).
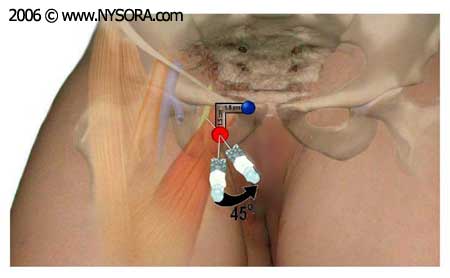
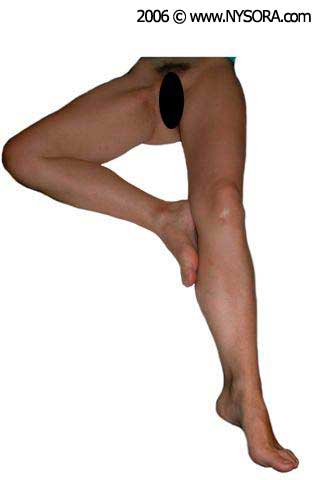
Paravascular selective inguinal block This technique consists of selective block of the two branches of the obturator nerve (anterior and posterior), performed at the inguinal level and slightly more caudad than the previously described techniques.[61] The femoral artery and the tendon of the long adductor muscle at the pubic tubercle are identified. For tendon identification, extreme leg abduction is required, Figure 10. A line is drawn over the inguinal fold from the pulse of the femoral artery to the tendon of the long adductor muscle. The needle is inserted at the mid-point of this line at an angle of 30º anterior/posterior and cephalically, Figure 11. By following the needle a few centimeters in depth, via the long adductor muscle, twitching responses from the long adductor and gracilis muscles are easily detectable on the posterior and medial aspect of the thigh. Subsequently, the needle is inserted deeper (0.5-1.5 cm) and slightly laterally over the short adductor muscle until a response from the major adductor muscle is obtained and can be visualized on the posterior-medial aspect of the thigh. Following needle insertion, infiltration of 5-7 ml local anesthetic is recommended. Occasionally, a more caudal division of the obturator nerve is found; hence, the two branches are located within the same location at the inguinal fold and two different motor responses may be observed with a single stimulation (injection).
Choice of Local Anesthetic Ten to 15 ml of local anesthetic is adequate in patients. The type and concentration of the local anesthetic depends upon the indication for the block. For diagnostic-therapeutic blockades, highly concentrated neurolytic solutions are utilized to achieve long lasting blocks. In the literature, combinations of phenol, ethanol, bupivacaine, levobupivacaine and/or steroids are well reported.[62-67] For lower limb surgeries, the recommended anesthetic technique consists of the administration of medium- to long-lasting local anesthetics that are associated with adequate postoperative analgesia such, as bupivacaine 0.25-0.5%; ropivacaine 0.25-0.75% and levobupivacaine 0.25-0.5%. To avoid adductor muscle spasms during transurethral surgery, the use of medium to long local anesthetics is not required as the surgery does not last more than 2 hours. Therefore mepivacaine 1-2% or lidocaine 1-2% should be adequate for this purpose.[68,69] Block Evaluation The onset of motor blockade is seen approximately 15 min after administration of 1% Mepivacaine, and 25 min following injection of 0.75% Ropivacaine. Evaluation of an obturator block by sensory testing is unreliable due to the variability in its sensory distribution (Figure 10). In some cases, the obturator nerve may not contain any sensory branches that can be clinically tested for adequacy of the blockade. In addition, even when a sensory branch is present, there is considerable overlap of cutaneous innervation from the obturator, femoral and sciatic nerves. It is often erroneously thought that the skin of the medial aspect of the thigh is innervated by the obturator nerve; in fact sensory branches of the femoral nerve contribute sensory innervation to this region.
The area of skin most commonly regarded as having exclusive obturator nerve supply is a small region located on the posteromedial aspect of the knee. Also, the strength of the lower limb adductors relies 70% on the obturator nerve. Consequently, reduction in the strength of the adductors of the thigh is the most reliable sign of successful obturator nerve blockade. Adductor muscle strength can be objectively evaluated by comparing the maximal pressure exerted by the patient squeezing a sphygmomanometer that has been pre-inflated to 40mmHg and placed between their legs, before and after block performance. Failure to demonstrate a reduction in adductor muscle strength from baseline is synonymous with block failure. Perioperative Management Patients must be warned that ambulation may be impaired due to the blockade of the thigh adductors. Complications There are no reports of complications associated with obturator nerve block. The lack of reported complications however, is more likely to the infrequent use of this block, rather then its inherent safety. Needle orientation for the classical pubic approach of Labat is towards the pelvic cavity. Therefore, if advanced too far in a cephalad direction, the needle can pass over the superior pubic ramus and penetrate the pelvic cavity, perforating the bladder, rectum and spermatic cord. Accidental puncture of the obturator vessels could result in unintentional intravasacular injection and hematoma formation. A retropubic anastamosis between the external iliac and obturator arteries (corona Mortis) is present in up to10% of patients: bleeding secondary to puncture of the corona Mortis can be difficult to control. Obturator neuropathy, secondary to needle trauma, intraneural injection, nerve ischemia or local anaesthetic toxicity are also possible, similarly to other peripheral nerve block techniques. REFERENCES: 1. Labat G: Regional Anesthesia: Its technic and clinical application. Philadelphia, Saunders Company, 1922. 2. Parks CR,Kennedy WF: Obturator nerve block: A simplified approach. Anesthesiology 28:775-778, 1967. 3. Wassef M: Interadductor approach to obturator nerve blockade for spastic conditions of adductor thigh muscles. Reg Anesth 18:13-17, 1993. 4. Pinnock CA, Fischer HBJ, Jones RP: Perepheral Nerve Blockade. New York, Churchill Livingstone, 1996. 5. Winnie AP, Ramamurthy S, Durrani Z: The inguinal paravascular technic of lumbar plexus anaesthesia: The "3-in-1" block. Anesth Analg 52:989-996, 1973. 6. Kim PS, Ferrante FM: Cryoanalgesia: a novel treatment for hip adductor spasticity and obturator neuralgia. Anesthesiology 89: 534-536, 1998. 7. Wheeler ME, Weinstein SL: Adductor tenotomy-obturator neurotomy. J Pediatr Orthop 4:48-51, 1984. 8. Benzel EC, Barolat-Romana G, Larson SJ: Femoral obturator and sciatic neurectomy with iliacus and psoas muscle section for spasticity following spinal cord injury. Spine 13:905-8, 1988. 9. Pelissier J: Chemical neurolysis using alcohol in the treatment of spasticity in the hemiplegic. Cah Anesthesiol 41;139-43, 1993. 10. Akat T, Murakami J, Yoshinaga A: Life-threaening haemorrhage following obturator artery injury during transurethral bladder surgery: a sequel of an unsuccessful obturator nerve block. Acta anaesthesiol Scand. 43:784-8, 1999. 11. Shulm MS: Simultaneous bilateral obturator nerve stimulation during transurethral electrovaporizacion of the prostate. J. Clin Anesth 10:518-21, 1998. 12. Prentiss RJ: Massive adductor muscle contraccion in transurethral surgery: Cause and prevention; development of new electrical circuit. Trans Am Assoc Genitourin Surg 56:64-72, 1964. 13. Shiozawa H: A new transurethral resection system: operating in saline environment precludes obturator nerve reflex. J Urol 168:2665-7, 2002. 14. Biserte J.: Treatment of superficial bladder tumors using the argon laser. Acta urol Belg. 57:697-701, 1989. 15. Brunken C, Qiu H, Tauber R: Transurethral resection of bladder tumours in physiological saline. Urologe 43:1101-5, 2004. 16. Hobika JH, Clarke BG: Use of neuromuscular blocking drugs to counteract thigh-adductor spasm induced by electrical shocks of obturator nerve during transurethral resection of bladder tumors. J Urol 85:295-6, 1961. 17. Atanassoff PG, Weiss BM, Brull SJ: Lidocaine plasma levels following two techniques of obturator nerve block. J Clin Anesth. 8: 535-9, 1996. 18. Kakinohana M: Interadductor approach to obturator nerve block for transurethral resection procedure: comparison with traditional approach. J Anesth 16:123-6, 2002. 19. Deliveliotis C, Alexopoulou K, Picramenos D, et al.: The contribution of the obturator nerve block in the transurethral resection of bladder tumor. Acta Urol Belg 63:51-4, 1995. 20. Schwilick R, Wingartner K, Kissler GV, et al.: Elimination of the obturator reflex as a specific indication for dilute solution of etidocaie. A study of the suitablility of a local anesthetic for reflex elimination in the 3-in-1 block technic. Reg Anesth 13:610, 1990. 21. Rubial M, Molins N, Rubio P, et al.: Obturator nerve block in transurethral surgery. Actas Urol Esp 13:79-81, 1989. 22. Gasparich JP,MasonJT, Berger RE: Use of nerve estimulator for simple and accurate obturator nerve block before transurethtral resection. J Urol 132:291-293, 1984. 23. Wassef M: Interadductor approach to obturator nerve blockade for spastic conditions of adductor thigh muscles. Reg Anesth 18:13-17, 1993. 24. Pelissier J: Chemical neurolysis using alcohol in the treatment of spasticity in the hemiplegic. Cah Anesthesiol 41;139-43, 1993. 25. Viel E, Pelissier J, Pellas F, et al.: Alcohol neurolytic blocks for pain and muscle spasticity. Neurochirurgie. 49:256-62, 2003. 26. Viel E.J, Peennou D, Ripart J, et al.: Neurolytic blockade of the obturator nerve for intractable spasticity of adductor thigh muscle. Eur J Pain. 6:97-104, 2002. 27. Kirazli Y, On AY, Kismali B, et al.: Comparison of phenol block and botulinus toxin type A in the treatment of spastic foot aster stroke. A randomized double-blind trial. Am J Phys Med Reahabil. 77:510-515, 1998. 28. Loubser PG: Neurolytic interventions for upper extremity spasticity associated with head injury. Reg Anesth 22:386-387, 1997. 29. Heywang-Kobrunner SH, Amaya B, Okoniewski M, et al.: CT-guided obturator nerve block for diagnosis and treatment of painful condicions of the hip. Eur Raiol. 11:1047-53, 2001. 30. Hong Y, O'Grady T, Lopresti D, et al.: Diagnostic obturator nerve block for inguinal and back pain : a recovered opinion. Pain. 67:507-9, 1996. 31. Edmonds-seal J, Turner A, Khodadadeh S, et al.: Regional hip blockade in osteoarthrosis. Effects on pain perception. Anaesthesia. 37:147-51, 1982. 32. James CDT, Little TF: Regional hip blockade. A simplified technique for the relief of intractable osteoarthritic pain. Anaesthesia 31:1060-1070, 1976. 33. Sunderland S. Obturator nerve, in Suderland S (ed): Nerves and nerve injuries. Edinburg, Livingstone Ltd, 1968: p 1096-109. 34. Whiteside JL, Walters MD: Anatomy of the obturator region: relations to a trans-obturator sling. Int Urogynecol J Pelvis Floor Dysfunt 15:223-6, 2004. 35. Falsenthal G: Nerve blocks in the lower extremities: Anatomic considerations. Arch Phys Med Rehabil 55:504-507, 1974. 36. Winnie AP, Ramamurthy S, Durrani Z: The inguinal paravascular technic of lumbar plexus anaesthesia: The “3-in-1" block. Anesth Analg 52:989-996, 1973. 37. Parkinson SK, Mueller JB, Little WL, et al.: Extend of blockade with various approaches to the lumbar plexus. Anesth Analg 68: 243-248, 1989. 38. Brindenbaugh PO, Wedel DJ. The lower extremity.Somatic blockage, in Cousins MJ,Brindenbaugh PO,(ed): Neural blockage in clinical anaesthesia and management of pain. Philadelphia, Lippincott-Raven, 1998; p 373-394. 39. Atanassoff PG, Weiss BM, Brull SJ, et al.: Electromyographic comparison of obturator nerve block to three-in-one block. Anesth Analg 81:529-533, 1995. 40. Ritter JW: Femoral nerve "sheath" forn inguinal paravascular plexus block is not found in human cadavers. J Clin Anesth 7:470-473, 1995. 41. Seeberger MD, Urwyler A: Paravascular lumvar plexus extension after femoral nerve situlation and injection of 20 vs 40 ml mepivacaine 10 mg/kg. Acta Anesthesia Scand 39:769-813, 1995. 42. Singelyn FJ, Gouverneur JM, Gribomont BF: A high posicion of the catheter increases the success rate of continuous 3-in-1 block. Anesthesiology 85:A723, 1996. 43. Capdevila X, Biboulet P, Morau D, et al.: Continuos 3-in-1 block for postoperative pain after lower limb orthopedic surgery: Where the catheter go? Anesth Analg 94:1001-1006, 2002. 44. Dalens B, Vanneuville G, Tanguy A: Comparison of the fascia iliac block with the 3-in-1 block in children. Anesth Analg 69:705-713, 1989. 45. Morau D, Lopez S, Biboulet P, et al.: Comparison of continuous 3-in-1 and fascia iliaca compartment blocks for postoperative analgesia : feasibility, catheter migration, distribution of sensory block, and analgesic efficacy. Reg Anesth Pain Med. 28:309-14, 2003. 46. Capdevila X, Biboulet P, Bouregba M, et al.: Compartment of the 3-in-1 and fascia iliaca compartment block in adults: Clinical and radiographic análisis. Anesth Analg 86:1039-1044, 1998. 47. Winnie AP, Ramamurthy S, Durrani Z, et al.: Plexus blocks for lower extremity surgery. Anesthesiol Rev 1:1-6, 1974. 48. Chayen D, Nathan H, Chayen M: The posterior compartment block. Anesthesiology 45:95-99, 1976. 49. Hanna MH, Peat SJ, D´Costa F: Lumbar pexus block: An anatomical study. Anaesthesia 48:675-678, 1993. 50. Schupfer G, Jöhr M: Psoas compartment block in children: Part I-description of the technique. Pediatric Anesth 15:461-64, 2005. 51. Pandin PC, Vandesteen A, d´Hollander AA: Lumbar plexus posterior aproach; A catheter placemente description using electrical nerve stimulation. Anesth Analg 95:1428-1431, 2002. 52. Awad IT, Duggan EM: Posterior lumbar plexus block: Anatomy, Approaches, and Techniques. Reg Anesth Pain Med 30:143-149, 2005. 53. Mansour NY: Reevaluating the sciatic nerv block: another landmark for consideration. Reg Anesth 18:322-3, 1993. 54. Morris GF, Lang SA, Dust WN, et al.: The parasacral sciatic nerv block. Reg Anesth 22:223-8, 1997. 55. Jochum D, Iohom G, Choquet, et al.: Adding a selective obturator nerve block to the parasacral sciatic nerve block : an evaluation. Anesth Analg. 99:1544-9, 2004. 56. Choquet O, Nazarian S, Manelli H. Bloc obturateur au pli inguinal : étude anatomique. Ann Fr Anesth Réanim 20: 131s, 2001. 57. Wassef M: Interadductor approach to obturator nerve blockade for spastic conditions of adductor thigh muscles. Reg Anesth 18:13-17, 1993. 58. Pelissier J: Chemical neurolysis using alcohol in the treatment of spasticity in the hemiplegic. Cah Anesthesiol 41;139-43, 1993. 59. Viel E, Pelissier J, Pellas F, et al.: Alcohol neurolytic blocks for pain and muscle spasticity. Neurochirurgie. 49:256-62, 2003. 60. Viel E.J, Peennou D, Ripart J, et al.: Neurolytic blockade of the obturator nerve for intractable spasticity of adductor thigh muscle. Eur J Pain. 6:97-104, 2002. 61. Kirazli Y, On AY, Kismali B, et al.: Comparison of phenol block and botulinus toxin type A in the treatment of spastic foot aster stroke. A randomized double-blind trial. Am J Phys Med Reahabil. 77:510-515, 1998. 62. Fujita Y, Kimura K, Furukawa Y, et al.: Plasma contentrations of lignocaine alter obturator nerve block combined with spinal anaesthesia in patient undergoing transurethral resection procedures. Br J Anaesth 68:596-8, 1992. 63. Loubser PG: Neurolytic interventions for upper extremity spasticity associated with head injury. Reg Anesth 22:386-387, 1997. 64. Atanassoff PG, Weiss BM, Brull SJ: Lidocaine plasma levels following two techniques of obturator nerve block. J Clin Anesth. 8: 535-9, 1996. |

 Facebook
Facebook
 del.icio.us
del.icio.us
 Digg
Digg
 StumbleUpon
StumbleUpon
More from Lower Extremity

Transgluteal / Anterior Approach
A B Figure 1-1: (A) Needle insertion for the transgluteal (posterior) approach to sciatic nerve block. (B) ...

Intertendinous / Lateral Approach
A B Figure 1-1: (A) Needle insertion for the popliteal intertendinous approach. (B) Needle insertion for lateral ...

Femoral Nerve Block
Figure 1: Needle insertion for femoral nerve block. Essentials Indications: surgery of the anterior thigh ...
Ankle Block
Figure 1: Needle insertion for saphenous nerve block of the ankle. Essentials Indications: surgery of ...
| 12/19/2015(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/24/2016 | |
| 10/01/2024 |
![[advertisement] gehealthcare](../../../files/banners/banner1_250x600/GEtouch(250X600).gif)
Image gallery











Post your comment