![[advertisement] concertmedical](../../../files/bk-nysora-ad.jpg)
Intercostal Block
|
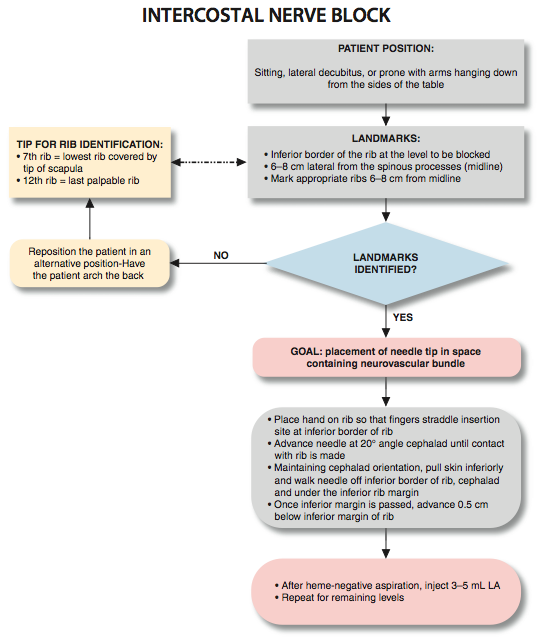
Figure 1: Intercostal nerve block: Patient position and needle insertion. Essentials
General Considerations Intercostal block produces discrete bandlike segmental anesthesia in the chosen levels. Intercostal block is an excellent analgesic option for a variety of acute and chronic pain conditions. The beneficial effect of intercostal blockade on respiratory function following thoracic or upper abdominal surgery, or following chest wall trauma, is well documented. Although similar in many ways to the paravertebral block, intercostal blocks are generally simpler to perform because the osseous landmarks are more readily palpable. However, the risks of pneumothorax and local anesthetic systemic toxicity are present, and care must be taken to prevent these potentially serious complications. Intercostal blocks can be more challenging to perform above the level of T7 because the scapula prevents access to the ribs. Although an intercostal block is an excellent choice for analgesic purposes, it is often inadequate as a complete surgical anesthesia. For this application, supplementation with another anesthesia technique usually is required. Regional Anesthesia Anatomy After emerging from their respective intervertebral foramina, the thoracic nerve roots divide into dorsal and ventral rami (Figure 2). The dorsal ramus provides innervation to the skin and muscle of the paravertebral region; the ventral ramus continues laterally as the intercostal nerve. This nerve then pierces the posterior intercostal membrane approximately 3 cm lateral to the intervertebral foramen and enters the subcostal groove of the rib, where it travels inferiorly to the intercostal artery and vein. Initially, the nerve lies between the parietal pleura and the inner most intercostal muscle. Immediately proximal to the angle of the rib, it passes into the space between the innermost and internal intercostal muscles, where it remains for much of the remainder of its course. At the midaxillary line, the intercostal nerve gives rise to the lateral cutaneous branch, which pierces the internal and external intercostal muscles and supplies the muscles and skin of the lateral trunk. The continuation of the intercostal nerve terminates as the anterior cutaneous branch, which supplies the skin and muscles of the anterior trunk, including the skin overlying the sternum and rectus abdominis.
Figure 2: Anatomy of the thoracic spinal and intercostal nerves. Distribution of Blockade  Figure 3: Injection of the local anesthetic (red dye) in intercostal space results in a medial-lateral spread of the local anesthetic in the intercostal space where the intercostal nerves (arrow) are contained. Intercostal blockade results in the spread of local anesthetic along the intercostals sulcus underneath the parietal pleura, leading to ipsilateral anesthesia of the blocked intercostals levels (Figure 3). A larger volume of local anesthetic or more medial injection may result in backtracking of local anesthetic into the paravertebral space. The extent of the resulting dermatomal distribution of anesthesia or analgesia is simply a function of the level of blockade. In contrast to paravertebral blockade, longitudinal (cephalad-caudad) spread between adjacent levels is much less common, although possible with large volumes of injectate and/or injection sites close to the midline of the back. In such instances, the local anesthetic can spread between the levels via the overflow into the paravertebral space. Single Injection Infraclavicular Block Equipment A standard regional anesthesia tray is prepared with the following equipment:
Figure 4: The patient position for intercostal block. A pillow is used as an abdominal/pelvic support. The arms are hanging off the table. Patient Positioning An intercostal block can be performed with the patient in the sitting, lateral decubitus, or prone positions. With the patient in sitting or lateral position, it is helpful to have the patient's spine arched with the arms extended forward. Patients who are prone are best positioned for the block by placing a pillow under the abdomen and with the arms hanging down from the sides of the bed (Figure 4). This rotates the scapulae laterally and permits access to the angles of the rib above the level of T7 (Figure 5). Landmarks and Maneuvers to Accentuate Them The following anatomic landmarks are used to estimate the position of the relevant ribs. 1. Twelfth rib (last rib palpable inferiorly) (Figure 6) 2. The 7th rib (lowest rib covered by the angle of the scapula) (Figure 7) Once identified by palpation, the inferior border of the corresponding ribs can be marked on the skin (Figure 8). An "x" at the angle of the rib identifies the site of needle insertion, usually about 6-8 cm from the midline. For thoracotomy or upper abdominal incisions, an estimate of the levels required for effective analgesia can be made after discussion with the surgeon as to the planned approach and length of incision. Analgesic blocks for rib fractures are planned based on the area of the injury. Typically, in addition to the estimated dermatomal levels, one additional level above and one below the estimated levels are also blocked.
 Figure 7: Estimating T7 level at the tip of the scapula. Technique After cleaning the skin with an antiseptic solution, 1-2 mL of dilute local anesthetic is infiltrated subcutaneously at each planned injection site. The fingers of the palpating hand should straddle the insertion site at the inferior border of the rib and fix the skin to avoid unwanted skin movement. A 1.5-in, 22-gauge needle is attached to a syringe containing local anesthetic via extension tubing and advanced at an angle of approximately 20° cephalad to the skin (Figure 9). Contact with the rib should be made at within 1 cm in most patients. While main- taining the same angle of insertion, the needle is walked off the inferior border of the rib as the skin is allowed to return to its initial position. Then the needle is advanced 3 mm below the inferior margin of the rib, with the goal of placing the tip in the space containing the neurovascular bundle (i.e., between the internal and innermost intercostal muscles). The end point for advancement should be the predetermined distance (3 mm). Following negative aspiration for blood or air, 3-5 mL of local anesthetic of insertion and the needle withdrawn. The process is repeated for the remaining levels of blockade.
Choice of Local Anesthetic It is usually beneficial to achieve longer-acting anesthesia or analgesia for intercostal blockade by using a long-acting local anesthetic. Systemic absorption of local anesthetic is high following an intercostal block, and careful consideration of the dose should precede the block performance to decrease the risk of systemic toxicity. Table 1 lists some commonly used local anesthetic solutions and their dynamics with this block.  Figure 8: The needle insertion site for intercostal space is labeled 5-7 cm lateral to the midline. Table 1: Choice of Local Anesthetic for Intercostal Block 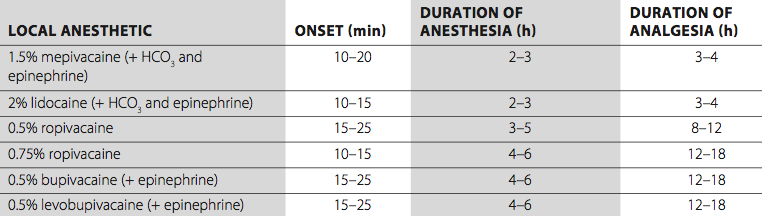 Block Dynamics and perioperative Management The performance of intercostal blocks is associated with relatively minor patient discomfort, although needle contact with the periosteum can be uncomfortable. A small dose of midazolam (2 mg) and alfentanil (250-500 µg) just before beginning the block procedure is usually adequate to decrease the discomfort. Excessive sedation should be avoided because positioning becomes difficult when patients cannot keep their balance in a sitting position. The first sign of successful blockade is the loss of pinprick sensation at the dermatomal distribution of the nerve being blocked. The higher the concentration and volume of local anesthetic used, the faster the onset.
Figure 9: The needle insertion site for intercostal space is labeled 5-7 cm lateral to the midline. Complications and how to Avoid Them Table 2 lists the complications of intercostal block and preventive techniques. It is usually beneficial to achieve longer-acting anesthesia or analgesia for intercostal blockade by using a long-acting local anesthetic. Systemic absorption of local anesthetic is high following an intercostal block, and careful consideration of the dose should precede the block performance to decrease the risk of systemic toxicity. Table 1 lists some commonly used local anesthetic solutions and their dynamics with this block. Table 2: Complications of Intercostal Block and Preventive Techniques 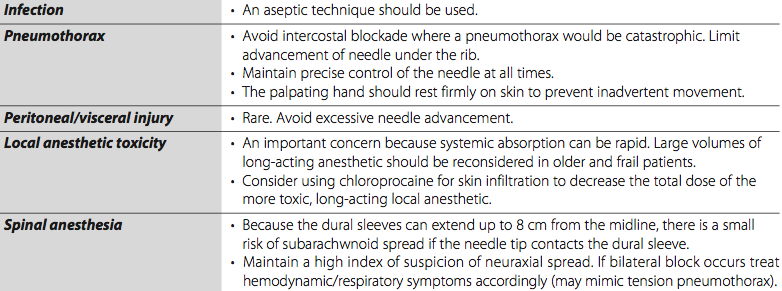
|

 Facebook
Facebook
 del.icio.us
del.icio.us
 Digg
Digg
 StumbleUpon
StumbleUpon
More from Landmark Based

Caudal Anesthesia
Caudal anesthesia was first described at the turn of last century by two French physicians, ...

Continuous Thoracic Paravertebral Block
Overview Indications: Breast surgery, pain management after thoracic surgery or rib fractures Landmarks: Spinal process at the desired ...

Thoraco Lumbar Paravertebral Block
Overview Indications: Inguinal hernia surgery, lateral abdominal wall surgery Landmarks: Spinal processes T9-L5 (the number and location of ...

Thoracic Paravertebral Block
Figure 1: Thoracic paravertebral block Essentials Indications: breast surgery, analgesia after thoracotomy or in patients with ...
Lumbar Plexus Block
Authors: Manoj Karmakar and Catherine Vandepitte Introduction Lumbar plexus block (LPB) traditionally is performed using surface anatomic ...

Spinal Anesthesia
Introduction with General Considerations & Brief History Carl Koller, an ophthalmologist from Vienna, first described the ...
| 02/20/2016(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/23/2016 | |
| 10/01/2024 |
![[advertisement] gehealthcare](../../../files/banners/banner1_250x600/GEtouch(250X600).gif)
Image gallery













Post your comment