![[advertisement] concertmedical](../../../files/bk-nysora-ad.jpg)
Ultrasound-Guided Interscalene Brachial Plexus Block
|
Figure 1: Ultrasound-guided interscalene brachial plexus block; transducer and needle position to obtain the desired ultrasound image for an in-plane approach. Essentials General Considerations  Figure 2: Relevant anatomy for interscalene brachial block and transducer position to obtain the desired views. Brachial plexus (BP) is seen sandwiched between middle scalene muscle (MSM) laterally and anterior scalene muscle (ASM) medially. Ultrasound image often includes a partial view of the lateral border of the sternocleidomastoid muscle (SCM) as well as the internal jugular vein (IJV) and carotid artery (CA). The transverse process of one of the cervical vertebrae is also often seen. The ultrasound-guided technique of interscalene brachial plexus block differs from nerve stimulator or landmark-based techniques in several important aspects. Most importantly, distribution of the local anesthetic is visualized to assure adequate spread around the brachial plexus. Ultrasound guidance allows multiple injections around the brachial plexus, therefore eliminating the reliance on a single large injection of local anesthetic for block success as is the case with non-ultrasound-guided techniques. Ability to inject multiple aliquots of local anesthetic also may allow for the reduction in the volume of local anesthetic required to accomplish the block. Repetition of the block in case of inadequate anesthesia is also possible, a management option that is unpredictable without ultrasound guidance. Finally, the risk of major vessel and nerve puncture during nerve block performance is reduced. Ultrasound Anatomy The brachial plexus at the interscalene level is seen lateral to the carotid artery, between the anterior and middle scalene muscles (Figures 2, 3, and 4). Prevertebral fascia, superficial cervical plexus and sternocleidomastoid muscle are seen superficial to the plexus. The transducer is moved in the superior-inferior direction until two or more of the brachial plexus trunks are seen in the space between the scalene muscles. Depending on the depth of field selected and the level at which the scanning is performed, first rib and/or apex of the lung may be seen. The brachial plexus is typically visualized at a depth of 1 to 3 cm. Distribution of Blockade The interscalene approach to brachial plexus blockade results in anesthesia of the shoulder and upper arm. Inferior trunk for more distal anesthesia can also be blocked by additional, selective injection, deeper in the plexus. This is accomplished either by controlled needle redirection inferiorly or by additional scanning to visualize the inferior trunk and another needle insertion and targeted injection.
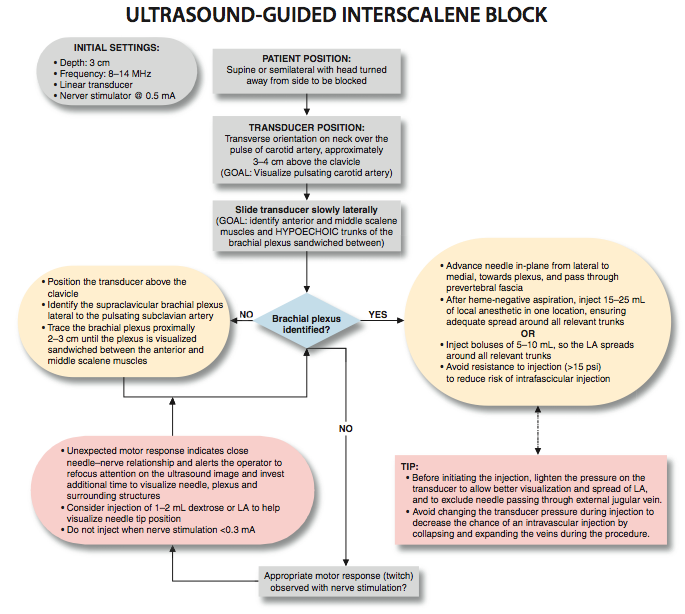
Equipment Equipment needed includes the following: Landmarks and Patient Positioning Any position that allows comfortable placement of the ultrasound transducer and needle advancement is appropriate. The block is typically performed with the patient in supine, semisitting, or semilateral decubitus position, with the patient's head facing away from the side to be blocked. The latter position may prove ergonomically more convenient, especially during an in-plane approach from the lateral side, in which the needle is entering the skin at the posterolateral aspect of the neck. A slight elevation of the head of the bed is often more comfortable for the patient, and it allows for better drainage and less prominence of the neck veins. Adherence to strict anatomic landmarks is of lesser importance for the ultrasound-guided interscalene block than it is the case for the surface anatomy-based techniques. Regardless, knowledge of the underlying anatomy and the position of the brachial plexus is important to facilitate recognition of the ultrasound anatomy. Scanning usually begins just below the level of the cricoid cartilage and medial to the sternocleidomastoid muscle with a goal to identify the carotid artery.
Technique With the patient in the proper position, the skin is disinfected and the transducer is positioned in the transverse plane to identify the carotid artery (Figure 5). Once the artery is identified, the transducer is moved slightly laterally across the neck (see algorithm at end of chapter). The goal is to identify the scalene muscles and the brachial plexus that is sandwiched between the anterior and middle scalene muscles. The needle is then inserted in-plane toward the brachial plexus, typically in a lateral-to-medial direction (Figure 7), although medial-to-lateral needle orientation also can be chosen if more convenient. As the needle passes through the prevertebral fascia, a certain "give" is often appreciated. When nerve stimulation is used (0.5 mA, 0.1 msec), the entrance of the needle in the interscalene groove is often associated with a motor response of the shoulder, arm, or forearm as another confirmation of the proper needle placement. After a careful aspiration to rule out an intravascular needle placement, 1 to 2 mL of local anesthetic is injected to document the proper needle placement (Figure 8A). Injection of several milliliters of local anesthetic often displaces the brachial plexus away from the needle. An additional advancement of the needle 1 to 2 mm toward the brachial plexus may be beneficial to assure a proper spread of the local anesthetic (Figure 8B). Whenever the needle is further advanced, or multiple injections used, assure that high resistance to injection is absent to decrease the risk of an intrafascicular injection. When injection of the local anesthetic does not appear to result in a spread around the brachial plexus, additional needle repositions and injections may be necessary. In an adult patient, 15 to 25 mL of local anesthetic is usually adequate for successful and rapid onset of blockade. Smaller volumes of local anesthetics can also be effective, however, their success rate in everyday clinical practice may be inferior to those reported in meticulously conducted clinical trials.
Continuous Ultrasound-Guided Interscalene Block The goal of the continuous interscalene block is similar to the non-ultrasound-based techniques: to place the catheter in the vicinity of the trunks of the brachial plexus between the scalene muscles. The procedure consists of three phases: needle placement, catheter advancement, and securing of the catheter. For the first two phases of the procedure, ultrasound can be used to assure accuracy. The needle is typically inserted in-plane from the lateral-to-medial direction and underneath the prevertebral fascia to enter the interscalene space (Figure 9), although other needle directions could be used.
Figure 9: Continuous brachial plexus block. Needle is inserted in the interscalene space using an in-plane approach. Please note that for better demonstration, sterile drapes are not used in the model in this figure.  Figure 10: An ultrasound image demonstrating needle and catheter (white arrow) inserted in the interscalene space between the anterior (ASM) and middle (MSM) scalene muscles. BP, brachial plexus.
Proper placement of the needle can also be confirmed by obtaining a motor response of the deltoid muscle, arm, or forearm (0.5 mA, 0.1 msec) at which point 4 to 5 mL of local anesthetic can be injected. This small dose of local anesthetic serves to assure adequate distribution of the local anesthetic as well as to make the advancement of the catheter more comfortable to the patient. This first phase of the procedure does not significantly differ from the single-injection technique. The second phase of the procedure involves maintaining the needle in the proper position and inserting the catheter 2 to 3 cm into the interscalene space in the vicinity of the brachial plexus (Figure 10). Insertion of the catheter can be accomplished by a single operator or with a helper. Proper location of the catheter can be determined either by visualizing the course of the catheter or by an injection of the local anesthetic through the catheter. When this proves difficult, alternatively, a small amount of air (1 mL) can be injected to confirm the catheter tip location. There is no agreement on what constitutes the ideal catheter securing system. The catheter is secured by either taping to the skin or tunneling. Some clinicians prefer one over the other. However, the decision about which method to use could be based on the patient's age, duration of the catheter therapy, and anatomy. Tunneling could be preferred in older patients with obesity or mobile skin over the neck and when longer duration of catheter infusion is expected. Two main disadvantages of tunneling are the risk of catheter dislodgment during the tunneling and the potential for scar formation. Fortunately, a number of catheter-securing devices are available to help stabilize the catheter.
|




 Facebook
Facebook
 del.icio.us
del.icio.us
 Digg
Digg
 StumbleUpon
StumbleUpon
More from Upper Extremity
Ultrasound-Guided Superficial Cervical Plexus Block
Figure 1: Needle and transducer position to block the superficial cervical plexus using a transverse ...

Ultrasound-Guided Infraclavicular Brachial Plexus Block
Figure 1: In-plane needle insertion technique during infraclavicular brachial plexus block. Essentials Indications: arm, elbow, forearm, and ...

Ultrasound-Guided Axillary Brachial Plexus Block
Figure 1: Transducer position and needle insertion in ultrasound-guided axillary brachial plexus block. Essentials Indications: forearm and ...
Ultrasound-Guided Forearm Block
A B C Figure 1: (A) Radial nerve block above the elbow. The needle is inserted in-plane from ...
Ultrasound-Guided Wrist Block
A B C Figure 1: Ultrasound-guided wrist block. Transducer and needle positions for (A) Median nerve block, (B) ...

Ultrasound-Guided Supraclavicular Brachial Plexus Block
Figure 1: Supraclavicular brachial plexus; transducer position and needle insertion. Essentials Indications: arm, elbow, forearm, and hand ...
| 02/20/2016(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/23/2016 | |
| 10/01/2024 |
![[advertisement] gehealthcare](../../../files/banners/banner1_250x600/GEtouch(250X600).gif)
Image gallery















Post your comment