![[advertisement] concertmedical](../../files/bk-nysora-ad.jpg)
February 2014 - Newsletter
In this issue: |
|
Dear NYSORA newsletter reader, February is an exciting month at NYSORA! We are getting ready to deploy the NYSORA Asia Educational Outreach Program in Katmandu, Nepal on March 2-3, followed by a program in Kuala-Lumpur, Malaysia on March 8-9. NYSORA Asia is currently in its 8th year of existence, providing didactic and hands on training to over 2000 anesthesiologists across Asia. Following the NYSORA Asia K2 mission, the NYSORA Latin America Collaborative Symposium will take place from March 14th to the 16th in beautiful Florianopolis, Brazil. The last day to save $50 on the registration fee for the NYSORA Latin America symposium is February 28. The last day to reserve a hotel room at the discounted rate is March 1st. NYSORA's first Latin American program is already proving to be a success!
Sincerely yours, Matt Becker |
||
|
|

|
The time is rapidly approaching for our very first NYSORA Latin America program in beautiful Florianopolis, Brazil. We have put together an amazing team of as many as 30 speakers from FIVE continents in building this valuable educational and networking program! Bringing this expertise to the doorstep of our colleagues in Latin America is truly an amazing endeavor. We are all thankful to Dr. Pablo Helayel and Dr. Carlos Bolini for their immense efforts in logistics and making this program a possibility. It wouldn't be a NYSORA event without blowing off a little steam. The Social Event, scheduled for Saturday, is a Luau Dinner at the Rancho do Pescador e Santinho Grill Restaurant at Costao do Santinho Resort Golf Spa, sponsored by Sonosite. NYSORA's Social Events are a great way to network with colleagues from around the globe.
We're happy to announce that the first NYSORA Latin America program will be packed! We were able to sponsor 12 qualifying scholars throughout Latin America under the NYSORA ESOP (Educational Scholarship Outreach Program). NYSORA has committed to providing complementary unrestricted access to all educational sessions and workshops, social programs as well as sponsoring housing for the ESOP scholars. The ESOP program is the cornerstone in NYSORA’s philanthropic effort.  NYSORA ESOP Scholars |
||
|
|


|
Techniques - A Scandal Rocks Our Choice of Antiseptic The patient safety world has recently been shaken by shame of insider payoffs (http://www.propublica.org/article/hidden-financial-ties-rattle-top-health-quality-group). In January, CareFusion settled allegations of violating the False Claim act paying the government 40.1 millions dollars (http://www.justice.gov/opa/pr/2014/January/14-civ-021.html). The payment resolved claims by the government that CareFusion paid 11.1 million dollars to influence favorable treatment and off labeled promotion for its ChloraPrep product. The evidence in these references is quite compelling.  How does this affect our choice of antiseptic solutions for the performance of regional anesthesia? In 2006, ASRA published guidelines giving a Grade A recommendation for using a chlorhexidine/alcohol-based product (http://www.asra.com/pdf/The-Importance-and-Implications.pdf). This was published prior to the FDA approval of an iodine/alcohol-based product. Since then, the evidence for which mixture performs best has shown conflicting results (http://www.ncbi.nlm.nih.gov/pubmed/23543526, https://www.ecri.org/Documents/Sample_Reports/Custom_Hotline_Response.pdf). At this time, it appears that either an iodine or chlorhexidine product mixed with alcohol could be considered optimal care. However, both of these solutions are considered off-labeled uses and its use should be judged in this context.  Paul H Willoughby MD Associate Professor of Clinical Anesthesiology Stony Brook University Medical Center |
|
|
|
Featured Education Video - Ultrasound-Guided Popliteal Block NYSORA Instructional video
|
|
|
|
Report from NYSORA Boutique Workshops For future dates, visit: NYSORA's Boutique Workshops 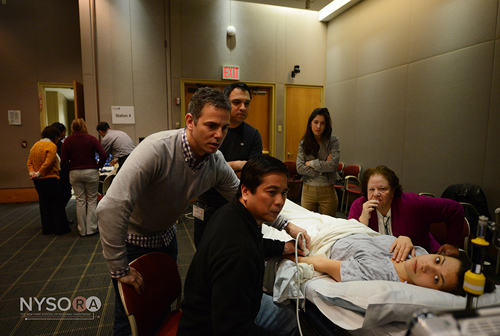 Dr. Jeff Gadsden instructing attendees With only a few months in existence, the NYSORA boutique workshops have become some of the most popular NYSORA educational programs. All three sessions to date have been fully booked and spaces are filling rapidly for the upcoming sessions in June, as well as the fall and winter of 2014. Keep an eye on NYSORA's CME offerings, as due to the high demand, we may introduce additional sessions. What makes NYSORA boutique workshops unique is a total focus on practical, hands-on, interactive teaching where the delegates have the opportunity to scan with all instructors, on all models and get their hands on anatomy. Moreover, models with larger BMI are also provided to better reflect actual clinical practice. A multitude of teaching tools are utilized - from live models to meat models, injection pressure models, peripheral vein access models, central vein access models to needle nerve guidance simulators. All practice sessions are preceded by an introduction highlighting the most pertinent functional regional anesthesia anatomy. After, the delegates are led through a step-by-step process on how to obtain, reproduce and utilize sonographic images to guide the needle placement in the six most common peripheral nerve block procedures. Delegates with more expertise are able to interact with our top international instructors and exchange experience and tips on how to improve efficiency, efficacy and safety of peripheral nerve blocks. Short focused sessions are presented on the safety aspects of peripheral nerve blocks and monitoring. In particular, the NYSORA teaching model focus is on utilizing the concept of depositing local anesthetic in the tissue space that contains the nerves while avoiding the controversies of intraneural, perineural etc. A full range of new teaching models are being developed for the March workshop dates aimed at substantially simplifying the techniques to allow a speedy transition from the beginner/analyses to an expert regionalist.  Example of NYSORA Teaching Model The image demonstrates an example of new NYSORA teaching models. Shown is a sketch of axillary brachial plexus block demonstrating relative relationship of the tissues that may be encountered during axillary brachial plexus block performance. Of essence to understanding the concept that axillary sheath (7&8) contains all nerves accept musculocutaneous (4). Such organization of the nerves in the axillary fossa explains why injection around the axillary artery is sufficient and simpler to accomplish the block rather than specific injections for specific nerves. This simplified approach substantially facilitates to block performance and cuts down on the time necessary to perform the block. The image also demonstrates why the use of nerve stimulation and injection pressure monitoring may be useful during axillary brachial plexus block to avoid the unnecessary needle nerve contact and/or intraneural injection. Since the axillary brachial plexus block is an injection of local anesthetic inside the neurovascular sheath, insertion of the needle into the sheets results in an injection of the local anesthetic in the adipose tissue of the axillary sheet. Such an injection should proceed without resistance, therefore injection pressures is always low (1-ulnar nerve, 2-median nerve, 3-radial nerve, 4-musculocutanous nerve, 5-humerus, 6-adipose tissue of the axillary fossa, 7 and 8-axillary neurovascular sheath. The local anesthetic injection occurs inside the sheath around the axillary artery (A). One or more axillary veins are always present within the sheath  Dr. Anna Lopez instructing at NYSORA |
|
|
|
NYSORA Conferences and Workshops
|
![]()
|
Needle and Injection Monitoring During Nerve Block Placement Sponsored by Macosta Medical USA |
|
|

 Facebook
Facebook
 del.icio.us
del.icio.us
 Digg
Digg
 StumbleUpon
StumbleUpon
| 12/19/2015(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/24/2016 | |
| 10/01/2024 |
![[advertisement] gehealthcare](../../files/banners/banner1_250x600/GEtouch(250X600).gif)
Post your comment