![[advertisement] concertmedical](../../files/bk-nysora-ad.jpg)
Continuous Peripheral Nerve Blocks in Outpatients
|
Introduction - Single-injection nerve blocks provide up to 16 hours of postoperative analgesia - Portable infusion pumps allow outpatients to receive continuous nerve blocks More than 40% of ambulatory patients experience moderate to severe postoperative pain at home following orthopedic procedures. (1) Up to 16 hours of analgesia may be provided by single-injection peripheral nerve blocks with long-acting local anesthetics. However, following block resolution, ambulatory patients must usually rely on oral opioids to control pain. Unfortunately, opioids are associated with undesirable side effects, such as pruritus, nausea and vomiting, sedation, and constipation. To improve postoperative analgesia following ambulatory surgery, there has been an increasing interest in providing "perineural local anesthetic infusions," also called, "continuous peripheral nerve blocks," to outpatients. This technique involves the percutaneous insertion of a catheter directly adjacent to the peripheral nerve(s) supplying the surgical site. Local anesthetic is then infused via the catheter providing potent, site-specific analgesia. Outpatients may theoretically experience the same level of analgesia previously afforded only to those remaining hospitalized by combining the perineural catheter with a portable infusion pump. In 1946, Ansbro first described continuous regional blockade using a cork to stabilize a needle placed adjacent to the brachial plexus divisions to provide a "continuous" supraclavicular block. (2) However, for decades patients were required to remain hospitalized because the available pumps used to infuse local anesthetic were large, heavy, and technically sophisticated. It was not until 52 years later that Rawal described outpatient perineural infusion using a percutaneous catheter and a small lightweight, portable infusion pump. (3) Advantages and Evidence - Significant decreases in postoperative pain and opioid side effects are possible. - Earlier home discharge is possible for a select subset of hospitalized patients. Following Rawal's article, case reports or series of ambulatory perineural infusion were described via catheters in various anatomic locations, including paravertebral, (4) interscalene, (5-7) intersternocleidomastoid, (8) infraclavicular, (6) axillary, (9) psoas compartment, (9,10) femoral, (9,11) fascia iliaca, (5) sciatic/Labat, (9,10) sciatic/popliteal, (6,12) and tibial nerve. (6) Ambulatory continuous peripheral nerve blocks in pediatric patients have also been reported in patients as young as 8 years of age. (13) However, Klein et al provided the first prospective evidence quantifying infusion benefits in 2000. (14) This randomized, double-masked, placebo-controlled investigation by Klein et al involved subjects undergoing open rotator cuff repair who received an interscalene block and perineural catheter preoperatively, and they were randomized to receive either perineural ropivacaine 0.2% or normal saline postoperatively (10 mL/h). Patients receiving perineural placebo averaged a 3 on a visual analog pain scale of 0 to 10, compared with a 1 for subjects receiving ropivacaine. Although a portable pump was used, patients remained hospitalized during local anesthetic infusion Data involving perineural infusion in outpatients were subsequently provided in four randomized double-masked, placebo-controlled studies. (15-18) Patients receiving perineural local anesthetic achieved both clinically and statistically significant lower resting and breakthrough pain scores compared with those using exclusively oral opioids for analgesia (Figure 1). In addition, they required dramatically fewer oral analgesics to achieve their improved level of analgesia (Figure 1). Preoperatively, subjects scheduled for moderately painful procedures had a perineural catheter placed: an infraclavicular catheter for hand/forearm procedures,(15) a popliteal catheter for foot/ankle surgeries,(16,18) or an interscalene catheter for shoulder procedures.(17) Postoperatively, patients received either perineural local anesthetic or normal saline and were followed at home for up to 60 hours. All patients were instructed to use a bolus from their infusion pump for breakthrough pain and oral analgesics if this maneuver failed. In patients with an interscalene catheter following shoulder surgery, the local anesthetic infusion provided analgesia so complete that 80% of patients receiving ropivacaine required one or fewer opioid tablets per day during their infusion, and they reported average resting pain Additional benefits related to improved analgesia were experienced by patients who received perineural local anesthetic. Of patients receiving perineural ropivacaine, 0 to 30% reported insomnia due to pain, compared with 60 to 70% of patients receiving placebo. (15-17) Additionally, awakenings from sleep because of pain averaged 0.0 to 0.2 times on the first postoperative night, compared with 2.0 to 2.3 times for patients using only oral opioids. (15-17) Using fewer opioid tablets was associated with a lower rate of nausea, vomiting, pruritus, and sedation. (15-18) Satisfaction with postoperative analgesia was both clinically and statistically higher for patients receiving local anesthetic. (15-18) Finally, patients with popliteal local anesthetic infusion rated their "quality of recovery" (0-100; 100 = highest) an average of 96 compared with 83 for patients receiving placebo. (18) Whether these demonstrated benefits result in an improvement in patients' health-related quality-of-life remains unexamined. (19) Also uninvestigated to date is the relative superiority of one location over another for similar procedures (e.g., axillary vs. infraclavicular for hand surgery). The possible advantages of using outpatient perineural infusion to allow earlier discharge of patients who require potent analgesia has only recently been explored. Individual benefits of a shorter hospitalization may include a decrease in nosocomial infection, (20,21) harmful medical errors, (22,23) and increases in health-related quality-of-life. (19) Societal benefits include a potentially enormous cost savings. (24-26) Using ambulatory perineural infusion, patients have been discharged home directly from the recovery room following total elbow (unpublished data, Ilfeld et al, 2004) and shoulder replacement, (27) and on the first post-operative day following total hip (unpublished data, Ilfeld et al, 2004) and knee replacement. (28) Additional data are required to define the appropriate subset of patients and assess the benefits and incidence of complications associated with this practice.
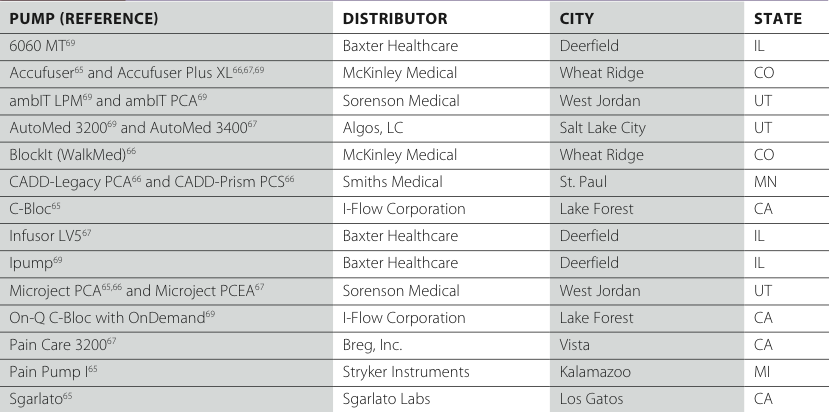
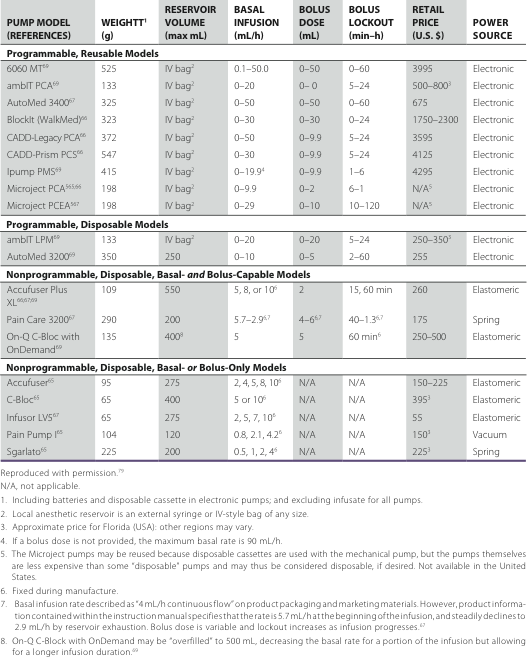
Figure 1: Effects of interscalene and sciatic/popliteal perineural infusion of either ropivacaine or placebo on average pain at rest (panels A and D), worst pain overall (panels B and E), and opiate use (panels C and F) following moderately painful shoulder or lower extremity surgery (scale: 0–10). Each opiate tablet consisted of oxycodone, 5 mg. Note: The infusion was discontinued after postoperative day 2 as indicated by the horizontal lines. Data are expressed as median (horizontal bar) with 25th-75th (box) and 10th-90th (whiskers) percentiles for patients randomly assigned to receive either 0.2% ropivacaine or 0.9% saline placebo. For tightly clustered data (e.g., panel A, postoperative days 0 and 1, ropivacaine group), the median approximated the 10th and 25th percentile values. In this case, the median is zero and only the 75th and 90th percentiles are clearly noted; p < 0.05: *, compared with saline for a given postoperative day. Reproduced with permission. (16,17) Patient Selection - Outpatient infusion is often limited to patients expected to have moderate pain. - Appropriate patient selection is crucial for safe outpatient infusion. Many investigators have limited the use of ambulatory infusion to patients who are expected to have moderate or severe postoperative pain >24 hours that is not easily managed with oral opioids. This practice is in an attempt to balance the potential benefits of this technique with the potential risks, (29,30) financial cost, and patient inconvenience of carrying an infusion pump and up to 600 mL of local anesthetic. (27) However, outpatient infusion may be used following mildly painful procedures defined here as usually well-managed with oral opioids to decrease opioid requirements and opioid-related side effects. (3,31) Appropriate patient selection is crucial for safe outpatient infusion because not all patients desire, or are capable of accepting, the extra responsibility that comes with the catheter and pump system. Because some degree of postoperative cognitive dysfunction is common following surgery, (32) patients are often required to have a "caretaker" during infusion. (15-17,33-36) Whether a caretaker is necessary for one night or for the entire duration of infusion remains unresolved. (37) If removal of the catheter is expected to occur at home, then a caretaker willing to perform this procedure must be available at the infusion conclusion if the patient is unwilling or unable to do this themselves (e.g., psoas compartment catheter). In medically unsupervised outpatients, complications may take longer to identify or be more difficult to manage than for hospitalized patients. Therefore, hepatic or renal insufficiency have been relative contraindications to outpatient infusion in an effort to avoid local anesthetic toxicity. (38) For infusions that may effect the phrenic nerve and ipsilateral diaphragm function (e.g., interscalene or cervical paravertebral catheters), patients with heart or lung disease are often excluded because continuous interscalene local anesthetic infusions have been shown to cause frequent ipsilateral diaphragm paralysis. (39) Conservative application of this technique is warranted until additional investigation of hospitalized medically supervised patients documents its safety, (40,41) although the effect on overall pulmonary function may be minimal for relatively healthy patients. (42) Selection of Insertion Technique - The optimal equipment and insertion techniques have yet to be determined. - A "test dose" of local anesthetic and epinephrine via the catheter is mandatory. - Securing the catheter adequately is of paramount concern. In a substantial number of cases-as high as 40% in some reports (43)-inaccurate catheter placement may occur. (17,44,45) This issue is of critical importance for outpatients because catheter replacement is not an option after leaving the medical facility. Many techniques and types of equipment have been described for catheter insertion. Using one common technique, the initial local anesthetic bolus is given via the needle, followed by catheter placement. However, using this method, it is possible to provide a successful surgical block but inaccurate catheter placement. (17) For ambulatory patients, the inadequate perineural infusion often will not be detected until after surgical block resolution following home discharge. (17) Using another technique, investigators have first inserted the catheter and then administered a bolus of local anesthetic via the catheter, with a reported failure rate of 1 to 8%.(46,47) In an attempt to further improve catheter-placement success rates, "stimulating" catheters have been developed that deliver current to the catheter tip. (48) This design provides feedback on the positional relationship of the catheter tip to the target nerve prior to local anesthetic dosing. (33,34) To date, there are no studies comparing stimulating and nonstimulating catheters. However, there is limited evidence that passing current via the catheter may improve the accuracy of catheter placement. (49) The optimal placement techniques and equipment for ambulatory perineural infusion have yet to be determined and require further investigation. (50) A local anesthetic and epinephrine "test dose" should be injected via the catheter in an effort to identify intrathecal, (51) epidural, (52) or intravascular (53) placement before infusion initiation, regardless of the equipment/technique used. Local Anesthetic and Adjuvant Selection - Most outpatient infusions reported involved ropivacaine or bupivacaine. - No adjuvant added to local anesthetic has been demonstrated to be of benefit. Although perineural infusions of levobupivacaine (54) and shorter-acting agents have been reported, (55-57) most publications have involved ropivacaine 0.2% or bupivacaine 0.125 to 0.25%. Currently, there is insufficient information to determine if there is an optimal local anesthetic (or concentration) for ambulatory infusions. (31,54,58) The optimal concentration and infusion rate for a particular catheter site in relationship to the degree of motor block has not been established either. Patient-Controlled Regional Analgesia - Providing patients the ability to self-administer bolus doses maximizes benefits - The optimal basal rate, bolus volume, and lockout time have not been determined. - Commonly used: basal 4-8 mL/h, bolus 2-5 mL, and lock- out time 20-60 minutes Available inpatient and outpatient data suggest that following procedures producing moderate to severe pain, providing patients with the ability to self-administer local anesthetic doses (patient-controlled regional analgesia) increases perioperative benefits and/or decreases local anesthetic consumption. (33,34,36,59-61) However, no information is available to base recommendations on the optimal basal rate, bolus volume, or lockout period, other than for interscalene catheters. (33) Until recommendations based on prospectively collected data are published, practitioners should be aware that investigators have reported successful analgesia using the following with long-acting local anesthetics: basal rate of 4 to 8 mL/h, bolus volume of 2 to 5 mL, and lockout duration of 20 to 60 minutes. Practitioners should be aware that the maximum safe doses for the long-acting local anesthetics remain unknown. However, multiple investigations involving patients free of renal or hepatic disease have reported blood concentrations within acceptable limits following up to 5 days of perineural infusion with similar dosing schedules. (38,62-64) Extrapolating from data involving patients receiving epidural bupivacaine infusion, a maximum infusion rate of 0.5 mg/kg per hour of bupivacaine may be considered. (38) Following ambulatory shoulder surgery with an interscalene catheter, infusion duration may be increased and similar baseline analgesia may be provided by decreasing the basal rate from 8 to 4 mL/h when patients supplement their block with large bolus doses (6 mL). (33) However, patients experience an increase in breakthrough pain incidence and intensity, sleep disturbances, and a decrease in satisfaction with their analgesia. Therefore, if ambulatory patients do not return for additional local anesthetic, practitioners are left with the dilemma of superior analgesia for a shorter duration versus a lesser degree of analgesia for a longer period of time. Of note, the infusion duration may be increased by progressively decreasing the basal infusion rate with a reprogrammable infusion pump, thus theoretically maximizing postoperative analgesia. (7) The publications that investigated the optimal dosing regimen for outpatients involved surgical procedures producing moderate postoperative pain. For procedures inducing mild postoperative pain, it is possible-even probable-that adequate analgesia would be adequately treated with a bolus-only dosing regimen. (31) There is also the possibility that stimulating catheters may be placed, on average, closer to the target nerve/plexus compared with nonstimulating devices. (49) If so, then the optimal dosing regimens, basal rates, and bolus doses may vary among different catheter types. Unfortunately, there are currently insufficient published data to draw any conclusions. Equipment - There is no one perfect infusion pump for all applications. - A multitude of factors must be taken into account when choosing a pump. Multiple small portable infusion pumps are currently available (Table 1; Figures 2 and 3), each with benefits and limitations (Table 2). Many factors must be taken into account when determining the optimal device for a given clinical situation. The provided list of infusion devices includes those for which performance data are available from independent sources and is not meant to be an exhaustive list of available units. Table 1: Infusion Pump Distributors
*reproduced with permission (79)
Bolus-Dose Capability Various pumps allow for both patient-controlled local anesthetic boluses and a basal infusion (Table 2); others allow for only one of these. (65-69) Bolus-dose capability (also termed patient-controlled regional analgesia, or PCRA) offers two significant benefits over continuous infusions alone. First, higher doses of oral opiates are often required for breakthrough pain without patient-controlled bolus doses. (34,68) Second, for outpatients using a limited local anesthetic reservoir, PCRA allows a provider to minimize the basal rate and, in turn, allows maximum infusion duration and minimal motor block (7) yet also permits bolus dosing for breakthrough pain (34) and physical therapy. (27,33,36,70) Compared with continuous infusions alone, equivalent or superior analgesia with a lower rate of local anesthetic consumption may be provided by using patient-controlled local anesthetic. (34,59-61) Disposability and Cost Reusable electronic infusion pumps are generally more expensive than the available single-use/disposable models (Table 2). However, reusable pumps that use relatively inexpensive disposable "cassettes" for each new patient (usually about US$10) may be more cost effective for practitioners who use these devices repeatedly (Table 2). But a reusable unit requires the patient to return the infusion pump by either the mail service or revisiting the surgical center. (33,34,36) Table 2: Infusion Pump Attributes
Patient Instructions - A prescription for oral opioids should be filled by patients following discharge. - Oral and written instructions, including health care provider contact numbers, should be provided. Following a single-injection nerve block for ambulatory surgery, discharge with an insensate extremity results in minimal complications. (71) However, whether or not patients should weight-bear with a continuous peripheral nerve block remains unexamined. Therefore, conservative management may be optimal, and some investigators have recommended that patients avoid using their surgical limb for weightbearing. (8,16,36) A prescription for oral analgesics should be provided to all patients, and the importance of filling the prescription immediately after leaving the surgical center should be emphasized. If patients wait to fill the prescription until after they have determined if oral analgesics are required, a period of inadequate analgesia may result. Most investigators educate both the patient and his or her caretaker at the same time before discharge because most patients have some degree of postoperative cognitive dysfunction. Both verbal and written instructions should be provided, along with contact numbers for health care providers who are available throughout the infusion duration. (6,15,31,72) In addition to standard outpatient instructions, topics reviewed often include expectations regarding surgical block resolution, infusion pump instructions, breakthrough pain treatment, catheter site care, limb protection, and the plan for catheter removal. Forewarning that pain in the operative limb is anticipated following surgical block resolution and fluid leakage at the catheter site is common-and what to do if these are experienced-often proves helpful. Signs and symptoms of possible catheter- and local anesthetic-related complications include, but are not limited to, pulmonary compromise, (40,41) nerve injury, (73) site infection, (74) and local anesthetic toxicity. (53) Although there are case reports of initially misplaced catheters, migration following a documented correct placement has not been described but remains a theoretical risk. (51-53,75,76) Possible complications of an unidentified initially misplaced catheter or of a catheter migration include intravascular or interpleural catheterization resulting in local anesthetic toxicity, intramuscular catheterization resulting in myonecrosis, and epidural/intrathecal catheterization when using interscalene, intersternocleidomastoid, paravertebral, or psoas compartment catheters. As is standard of care for inpatients, health care providers may want to consider documenting each patient contact (Figure 4). Catheter removal may be achieved with various techniques: Patients may be discharged with written instructions, (12) a health care provider may perform this procedure, (77) or patients' caretakers (or occasionally the patients themselves) may remove the catheters with instructions given by a provider over the telephone. (15-17,33,34,36) Although one technique has not been demonstrated to be superior to the others, one survey revealed that with instructions given by phone, 98% of patients felt comfortable removing their catheter at home. (78) Of note, only 4% would have preferred to return for a health care provider to remove the catheter, and 43% responded they would have felt comfortable with exclusively written instructions. (78) Nonsterile gloves may be provided for patients having their catheters removed at home. (15-17) 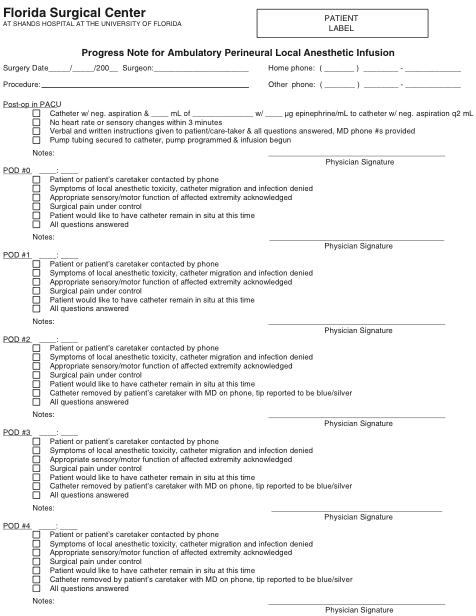
Figure 4: An example of a progress note that may be used to record telephone contacts with ambulatory patients. Reproduced with permission. (79)
     |
 Facebook
Facebook
 del.icio.us
del.icio.us
 Digg
Digg
 StumbleUpon
StumbleUpon
More from Foundations of RA

Equipment for Peripheral Nerve Blocks
Ali Nima Shariat, Patrick M. Horan, Kimberly Gratenstein, Colleen McCally, and Ashton P. Frulla Introduction ...

Indications for Peripheral Nerve Blocks
AUTHOR: Jeff Gadsden Introduction During the past 20 years, increasing knowledge in functional regional anesthesia anatomy, coupled ...
Neurologic Complications of Peripheral Nerve Blocks
Author: Jeff Gadsden Nerve injury following peripheral nerve blockade (PNB) is a potentially devastating complication that ...

Toxicity of Local Anesthetics
AUTHORS: Steven Dewaele, Alan C. Santos Introduction Systemic toxicity of local anesthetics can occur after administration of ...

Essentials of Regional Anesthesia Anatomy
--- Authors: Admir Hadzic and Carlo Franco A good practical knowledge of anatomy is important ...
Monitoring and Documentation
AUTHOR: Jeff Gadsden Introduction The incidence of complications from general anesthesia has diminished substantially in recent ...
Local Anesthetics: Clinical Pharmacology and Rational Selection
Author: Jeff Gadsden Local anesthetics (LAs) prevent or relieve pain by interrupt- ing nerve conduction. They ...

Electrical Nerve Stimulators and Localization of Peripheral Nerves
Ali Nima Shariat, Patrick M. Horan, Kimberly Gratenstein, Colleen McCally, and Ashton P. Frulla History of ...
| 02/20/2016(+ 2016 Dates) | |
| 01/27/2016 | |
| 03/17/2016 | |
| 04/20/2016 | |
| 09/23/2016 | |
| 10/01/2024 |
![[advertisement] gehealthcare](../../files/banners/banner1_250x600/GEtouch(250X600).gif)
Image gallery











Post your comment